

Background: Lisocabtagene maraleucel (liso-cel) is an investigational, CD19-directed, defined composition, 4-1BB chimeric antigen receptor (CAR) T cell product administered at equal target doses of CD8+ and CD4+ CAR+ T cells. Liso-cel is being studied in patients with relapsed/refractory (R/R) chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) in the ongoing, open-label, phase 1/2 TRANSCEND CLL 004 study (NCT03331198). Here, we report outcomes of patients in the phase 1 monotherapy cohort after a median follow-up of 18 months (mo).
Methods: Eligible patients had received ≥3 (standard-risk disease) or ≥2 (high-risk disease: del[17p], TP53 mutation, unmutated IGHV, or complex karyotype) lines of prior therapy, including a Bruton tyrosine kinase inhibitor (BTKi) unless contraindicated. Patients with active untreated central nervous system disease, Eastern Cooperative Oncology Group performance status >1, or Richter transformation were excluded. After 3 days of lymphodepletion with fludarabine and cyclophosphamide, patients received liso-cel infusion at 1 of 2 dose levels (DLs): 50 × 106 (DL1) or 100 × 106 (DL2) CAR+ T cells. Dose-limiting toxicities were evaluated for 28 days postinfusion. Responses were assessed using 2018 International Workshop on CLL criteria. Minimal residual disease (MRD) was assessed in blood by flow cytometry and/or in bone marrow (BM) by next-generation sequencing (both with a sensitivity of ≤10-4). Persistence of liso-cel was monitored by quantitative polymerase chain reaction.
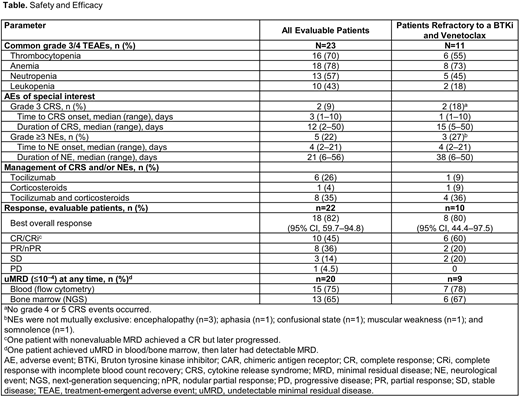
Results: Overall, 23 and 22 patients were evaluable for safety and efficacy, respectively. Median age was 66 (range, 49‒79) years, median number of prior therapies was 6 (range, 3‒13), and 83% of patients (n=19/23) had high-risk disease. All patients (N=23) had received prior ibrutinib, with 91% (n=21) refractory to, or who relapsed on, ibrutinib and 9% (n=2) who were intolerant to ibrutinib; overall, 48% (n=11) were refractory to both a prior BTKi and venetoclax. The safety profile was similar to that previously reported; no late or delayed adverse events of concern have emerged with the longer follow-up (Table). Among the 22 efficacy-evaluable patients, overall response rate (ORR; complete response [CR]/CR with incomplete blood count recovery [CRi] + partial response) was 82% (n=18); the CR/CRi rate was 45% (n=10). By Day 30, 68% of patients (n=15) achieved an overall response. At 15 mo and 18 mo, 53% (n=10/19; 6 CRs) and 50% (n=7/14; 5 CRs) of patients maintained their responses, respectively. At a median follow-up of 18 mo, the median duration of response was not reached (NR) in patients who had achieved a response to liso-cel (n=18), and median progression-free survival was 18 mo (95% CI, 3.0-NR) in all efficacy-evaluable patients. Two patients who completed the study maintained their response through 24 mo on study and have enrolled in a long-term follow-up study. Five of 8 patients who progressed had Richter transformation. The subgroup of patients refractory to both a prior BTKi and venetoclax had a similar ORR compared with the total evaluable population, with a CR rate of 60% (n=6/10; Table). Of 20 MRD-evaluable patients, 15 (75%) had undetectable MRD (uMRD) in the blood, 13 (87%) of whom also had uMRD in the BM, with most (60%) achieving uMRD in the BM by Day 30. Preliminary data show that liso-cel was detectable in the blood for up to 18 mo postinfusion in 4 (36%) of 11 patients.
Conclusions: Liso-cel treatment resulted in a high rate of uMRD in this heavily pretreated, high-risk population of patients with R/R CLL/SLL, including those refractory to both a BTKi and venetoclax. Responses were rapid and durable, with liso-cel detectable for up to 18 mo postinfusion. No late or delayed adverse events of concern emerged with longer follow-up. The phase 2 monotherapy expansion of the study is currently enrolling at DL2.
Siddiqi:AstraZeneca: Other: Travel/accommodations/expenses; Pharmacyclics LLC, an AbbVie Company, Seattle Genetics, Janssen, and AstraZeneca: Speakers Bureau; Juno: Membership on an entity's Board of Directors or advisory committees; Kite: Membership on an entity's Board of Directors or advisory committees; Pharmacyclics LLC, an AbbVie Company, Juno Therapeutics, KITE Pharma, AstraZeneca, TG Therapeutics, Celgene, Oncternal, and BeiGene: Research Funding; PCYC: Membership on an entity's Board of Directors or advisory committees; Astrazenca: Membership on an entity's Board of Directors or advisory committees; Celgene: Membership on an entity's Board of Directors or advisory committees; BeiGene: Other: DMC member; Juno Therapeutics, Pharmacyclics LLC, an AbbVie Company, AstraZeneca, Celgene, Kite Pharma, and BeiGene: Consultancy. Soumerai:Genentech/Roche: Research Funding; BostonGene: Research Funding; Beigene: Consultancy, Research Funding; GlaxoSmithKine: Research Funding; TG Therapeutics: Research Funding; AbbVie: Consultancy; AstraZeneca: Consultancy; Verastem: Consultancy. Dorritie:Kite-Gilead: Research Funding; Juno Therapeutics: Research Funding. Stephens:Beigene: Consultancy; Acerta: Research Funding; MingSight: Research Funding; Arqule: Research Funding; Verastem: Research Funding; Janssen: Consultancy; Juno: Research Funding; Gilead: Research Funding; Karyopharm: Consultancy, Research Funding; Pharmacyclics: Consultancy; Innate: Consultancy. Riedell:Karyopharm Therapeutics: Honoraria; Bayer: Honoraria; Kite Pharmaceuticals/Gilead: Honoraria, Research Funding; Novartis: Consultancy, Honoraria, Research Funding; Verastem Oncology: Honoraria; Celgene/Bristol-Myers Squibb Company: Honoraria, Research Funding; Morphosys: Research Funding. Arnason:Juno: Consultancy; Regeneron: Consultancy. Kipps:Pharmacyclics/ AbbVie, Breast Cancer Research Foundation, MD Anderson Cancer Center, Oncternal Therapeutics, Inc., Specialized Center of Research (SCOR) - The Leukemia and Lymphoma Society (LLS), California Institute for Regenerative Medicine (CIRM): Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Ascerta/AstraZeneca, Celgene, Genentech/F. Hoffmann-La Roche, Gilead, Janssen, Loxo Oncology, Octernal Therapeutics, Pharmacyclics/AbbVie, TG Therapeutics, VelosBio, and Verastem: Membership on an entity's Board of Directors or advisory committees; Oncternal Therapeutics, Inc.: Other: Cirmtuzumab was developed by Thomas J. Kipps in the Thomas J. Kipps laboratory and licensed by the University of California to Oncternal Therapeutics, Inc., which provided stock options and research funding to the Thomas J. Kipps laboratory, Research Funding; Genentech/Roche: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; VelosBio: Research Funding; Celgene: Honoraria, Research Funding; Gilead: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau. Gillenwater:Bristol-Myers Squibb: Current equity holder in publicly-traded company; Juno Therapeutics, a Bristol-Myers Squibb Company: Current Employment. Gong:Juno Therapeutics, a Bristol-Myers Squibb Company: Current Employment; Bristol-Myers Squibb: Current equity holder in publicly-traded company. Yang:Bristol-Myers Squibb: Current equity holder in publicly-traded company; Juno Therapeutics, a Bristol-Myers Squibb Company: Current Employment. Ogasawara:Bristol-Myers Squibb: Current equity holder in publicly-traded company; Bristol-Myers Squibb: Current Employment.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal